A guy starts testosterone replacement therapy. His energy comes back. His mood improves. He’s sleeping better, lifting heavier, feeling like himself for the first time in years.
Then his clinic runs labs and his estrogen is slightly elevated.
So they hand him an aromatase inhibitor. An estrogen blocker. Standard protocol, they tell him. Everyone gets one.
Within weeks, his joints ache. His mood tanks. Erections that had just come back? Gone again.
He went from feeling great to feeling worse than before he started TRT. And the hormone that was supposed to be the problem, estrogen, was actually doing its job.
The Estrogen Panic
Social media and testosterone clinics have turned estrogen into a villain for men. Scroll through any fitness forum or TRT subreddit and you’ll find men obsessing over their estradiol numbers the way they obsess over their bench press. High estrogen is framed as the enemy. Something to crush immediately.
The fear makes sense on the surface. Testosterone converts to estrogen through an enzyme called aromatase. More testosterone means more conversion. And estrogen in excess can cause real problems for men. Mood swings. Water retention. Gynecomastia.
But “can cause problems in excess” has been twisted into “must be eliminated.” That’s where the damage happens.
Plenty of men are walking around on estrogen blockers they never needed. They started TRT, their clinic reflexively added an aromatase inhibitor to the protocol, and nobody stopped to ask whether the man was actually having symptoms from elevated estrogen in the first place.
Colin Renaud, PA-C, who has treated hundreds of men on testosterone therapy, puts it directly: “We do NOT want to lower estrogen too much. Most men do not need estrogen blockers.”
What Estrogen Actually Does in Men
Estrogen gets dismissed as a hormone men don’t need. Wrong.
Men produce estrogen naturally. Their bodies need it. At appropriate levels, estrogen is responsible for some functions that most men would consider non-negotiable.
Mood stability. Estrogen helps regulate neurotransmitters in the brain. Tank a man’s estrogen and he’ll often become irritable, anxious, or flat. The emotional stability that came with starting TRT can vanish if estrogen drops too low.
Erection quality. This one surprises people. Renaud educates his patients on it constantly: “Believe it or not, men need estrogen to maintain and get an erection.” Men crash their estrogen thinking it will improve sexual function. The opposite happens.
Bone health. Estrogen plays a direct role in maintaining bone density in men. Chronically low estrogen contributes to osteoporosis, a condition most men don’t think about until a fracture forces them to.
Cardiovascular protection. Estrogen supports healthy vascular function. Suppressing it unnecessarily removes a layer of protection that the body put there on purpose.
Some of the top providers in the functional and integrative medicine space are now saying the goal should be to optimize estrogen in men, not suppress it. The old “lower it at all costs” mindset is outdated. The science and the clinical outcomes don’t support it.
When Estrogen Becomes a Problem (and When It Does Not)
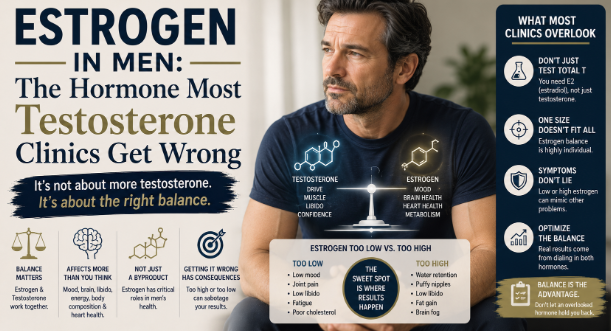
There are legitimate situations where estrogen is too high and intervention is appropriate. Symptoms of genuine estrogen excess in men include significant water retention, nipple sensitivity or tenderness, emotional instability that doesn’t match anything happening in their life, and in more pronounced cases, gynecomastia.
Note the word: symptoms.
A number on a lab report, by itself, is not an automatic reason to intervene. Renaud is clear about this: “Unless a man is symptomatic of high estrogen, if his estrogen is a little bit on the high side on labs or even out of range high but he feels good, don’t care. Leave it alone.”
That’s a critical distinction. Labs matter. Monitoring matters. But the man sitting in front of the provider matters more. If his estrogen is technically elevated but he feels strong, sleeps well, has a healthy sex drive, and his mood is stable, that number might just be where his body functions best.
Every man’s physiology is different. The ratio between testosterone and estrogen that produces the best outcomes varies from person to person. Forcing everyone into the same lab range ignores that reality.
Estrogen does become a real concern when testosterone doses are too high. Too much testosterone means too much aromatase conversion, which floods the body with estrogen. The fix there isn’t adding a blocker. The fix is adjusting the testosterone dose. Treat the cause, not the downstream effect.
The Cookie-Cutter Testosterone Clinic Problem
Here is where things go sideways for a lot of men.
Testosterone-only clinics have exploded in the last decade. Many of them operate on a simple model: man walks in, bloodwork confirms low T, man gets a standardized testosterone dose. Along with it, almost every patient gets an aromatase inhibitor. Same dose. Same protocol. Same pill bottle.
Renaud sees the results of this approach regularly, because men who started at those clinics often end up in his office looking for answers. “No disrespect, but a lot of times what’s happening is they’re just giving a very standardized dose of testosterone for any guy that walks in the door.”
The problem is obvious once you think about it. A 35-year-old athlete with 12 percent body fat and a 58-year-old with insulin resistance, 40 pounds of excess weight, and prediabetes are going to metabolize testosterone completely differently. Their aromatase activity will be different. Their estrogen response will be different. Treating them identically makes no clinical sense.
The one-size-fits-all estrogen blocker is the most common casualty of this approach. Men who felt great on testosterone start feeling terrible once their estrogen gets suppressed. Joints dry out. Libido crashes. Mood deteriorates. Some of them quit TRT entirely, thinking the testosterone was the problem. It wasn’t. The unnecessary blocker was the problem.
A Smarter Approach
Managing estrogen in men on TRT is not complicated. It just requires attention and patience.
Start with monitoring. Check estradiol alongside testosterone at every lab draw. Know the baseline. Track trends over time. Twice-yearly monitoring is standard once a man is stable on his dose.
Observe symptoms first. A slightly elevated estradiol in a man who feels excellent is not a crisis. It’s information. Document it. Watch it. Don’t react to it reflexively.
Intervene only when clinically necessary. If a man develops actual symptoms of estrogen excess (not just a number that looks high on paper) then intervention is appropriate. And even then, the first move should be evaluating whether the testosterone dose itself is too high.
Address the root drivers. Aromatase activity doesn’t happen in a vacuum. Body fat is one of the biggest factors. Fat tissue contains aromatase enzymes. More body fat means more testosterone-to-estrogen conversion. Insulin resistance amplifies this. A man carrying significant visceral fat and dealing with metabolic dysfunction will aromatize more aggressively than a lean, insulin-sensitive man on the same dose.
Gynecomastia, the physical sign men fear most, correlates with overproduction of both estrogen and prolactin. And that overproduction correlates with insulin resistance. The breast tissue isn’t the disease. It’s a downstream signal of metabolic dysfunction that needs to be addressed at its source.
So the real estrogen management protocol for men on TRT looks less like “hand everyone a pill” and more like this: get body composition right, improve insulin sensitivity, dose testosterone appropriately, monitor labs, and only reach for an aromatase inhibitor when a specific patient has specific symptoms that warrant it.
Sleep, stress management, diet, and exercise aren’t afterthoughts in estrogen management. They’re the foundation. A man who loses 30 pounds of body fat, cleans up his diet, and starts lifting heavy will often see his estrogen normalize on its own without touching his TRT protocol.
The Takeaway
Estrogen is not the enemy. It is an essential hormone in every man’s body, whether he’s on TRT or not.
The reflexive suppression of estrogen in men on testosterone therapy has caused real harm. Men losing erections. Men tanking their mood. Men quitting TRT because they felt worse on it, not realizing the blocker they didn’t need was the culprit.
If you’re on TRT and someone hands you an estrogen blocker without asking how you feel, without checking whether you’re actually symptomatic, ask why. Ask what specific symptoms they’re treating. Ask if the testosterone dose should be adjusted first.
A lab number alone is not a diagnosis. Your body is not a spreadsheet.
Find a provider who treats you as an individual, not a protocol.
About the Author: Colin Renaud, PA-C practices at Med Matrix (medmatrixusa.com), a functional medicine clinic in South Portland, Maine. With fellowship training in functional medicine and over a decade of experience in hormone optimization, he takes a personalized, evidence-based approach to testosterone therapy that goes far beyond a single lab number.